Mohs Surgery
Mohs micrographic skin cancer surgery or simply “Mohs surgery” is named after the surgeon, Dr. Frederic E. Mohs, who developed this innovative procedure. This precise form of skin cancer excision is the gold standard for removal of some of the most challenging skin malignancies located in the most sensitive regions such as the face, hands, feet and genitals. For these tumors Mohs surgery attains the highest cure rates achievable with studies demonstrating skin cancers are completely eradicated in 97 to 99% of cases.
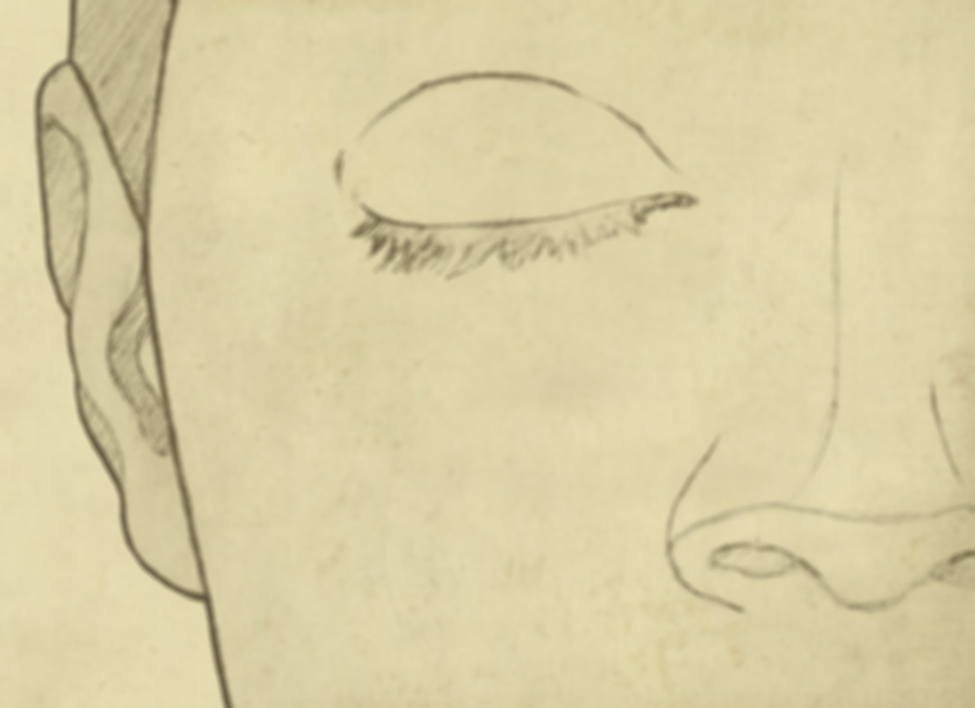
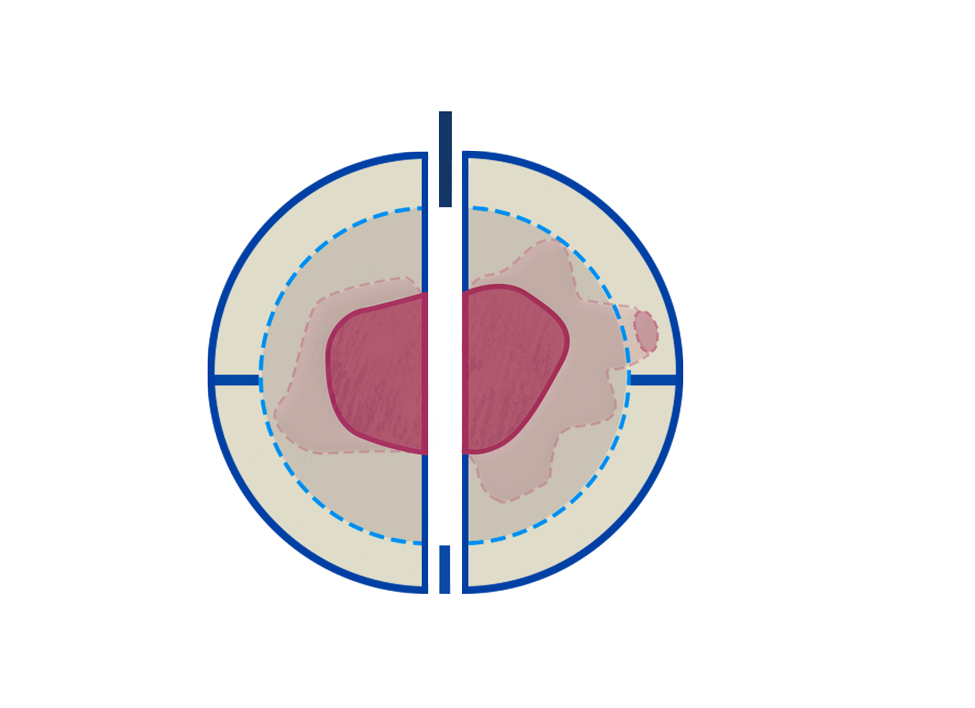
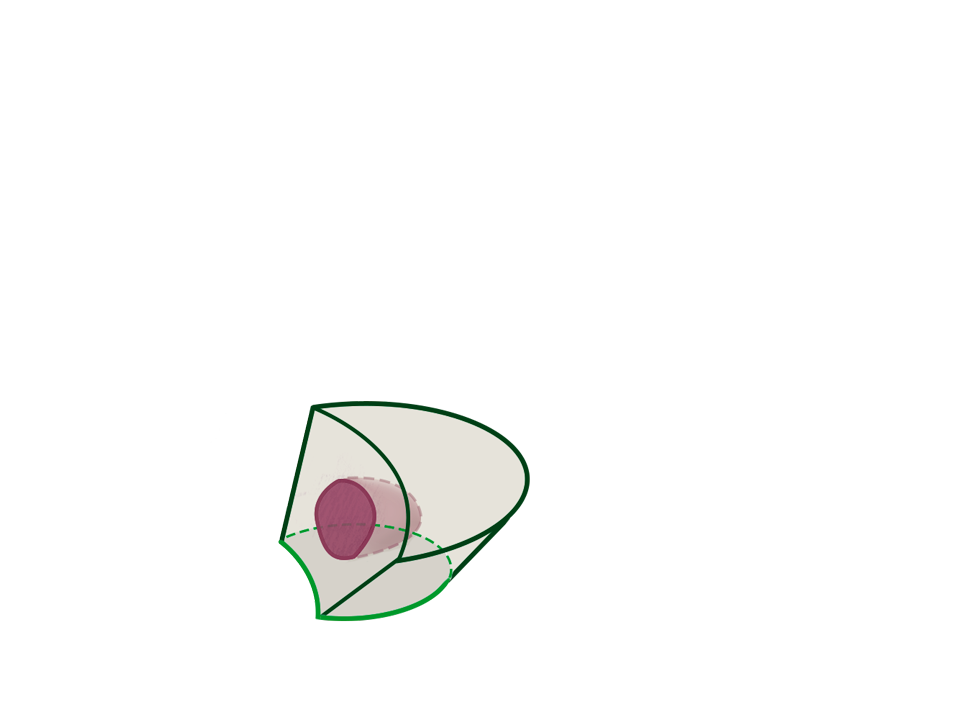
Figure 1
In the illustration to the left, the patient demonstrates a skin cancer in the cosmetically sensitive area below her right eye.